Why readings vary
Blood pressure moves up and down, even under anesthesia.
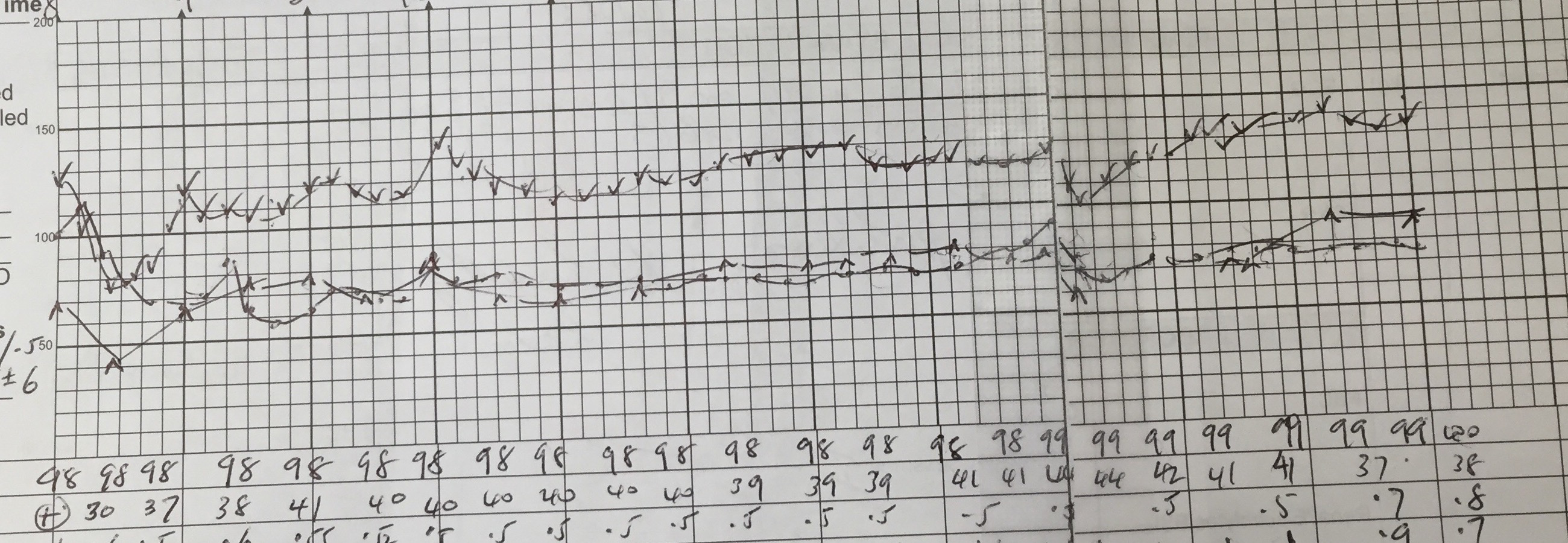
A blood pressure reading is a snapshot, not a permanent label. During a long operation, anesthetists chart blood pressure repeatedly and the trace still rises and falls with anesthesia depth, medicines, fluid shifts, bleeding, surgical stimulation, positioning, and recovery. Awake blood pressure also varies with posture, pain, exercise, stress, caffeine, alcohol, sleep, meals, a full bladder, and measurement technique.
That is why clinicians usually care about the pattern: repeated readings, home averages, ambulatory monitoring, and whether high numbers are linked with organ strain. One surprising reading deserves attention; a repeated pattern deserves a plan.
Intraoperative anesthetic charts make visible the same physiologic principle behind outpatient BP interpretation: pressure is dynamic. Induction, nociceptive stimuli, anesthetic depth, ventilation, volume status, blood loss, vasoactive agents, neuraxial effects, temperature, and surgical phase can move SBP/DBP substantially over minutes.
For chronic hypertension, avoid overinterpreting isolated values. Use standardized technique, average readings, HBPM/ABPM where useful, timing context, medication adherence, orthostatic symptoms, nocturnal pattern, and end-organ phenotype to decide whether the patient has sustained hypertension, white-coat effect, masked hypertension, or labile BP on top of true risk.
Body stateSleep, pain, stress, temperature, posture, hydration, and activity.
SubstancesCaffeine, nicotine, alcohol, stimulants, decongestants, and NSAIDs.
TechniqueCuff size, arm height, talking, rest time, and device validation.
PatternAverages and context are more meaningful than one number.




{kind=link}
{kind=link}
{kind=link}